Asthma is a long-term condition that affects your airways (bronchus - the tubes that carry air in and out of our lungs). The asthmatic airways are somewhat ‘sensitive’ and ‘inflamed’ and ready to react to a variety of stimuli (also known as triggers) when they come in contact. These triggers may be allergic or non allergic in nature. There is a familial trend in asthma as it is known to run in families especially with a history of allergies or smoking. The genetic basis of asthma is still being explored but there is some evidence that asthma in parents is a risk factor for asthma in their children.
Asthma video
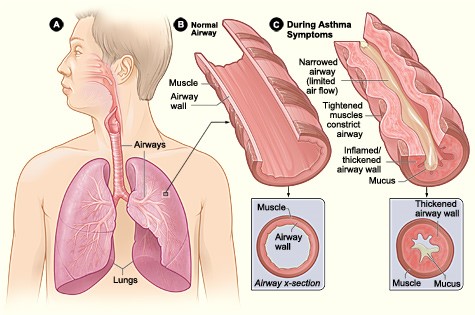
How does asthma affect the airways?
In an asthmatic individual, asthma triggers affects their airways in different ways that collectively result in the classic symptoms of asthma like shortness of breath, chest tightness, coughing and wheezing
The muscles around the walls of the airways tighten so that the airways become narrower
The lining of the airways becomes inflamed and starts to swell
Sticky mucus or phlegm sometimes builds up, which can narrow the airways even more
Who gets asthma?
Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals. The prevalence of asthma is increasing in many countries, especially in children. In the UK alone, a staggering 5.4 million people have been labelled as asthmatic. This translates to 1 in every 12 adults and 1 in every 11 children. In childhood, asthma affects more boys than girls and in adults, asthma is more common in women than men. Individuals employed in some occupations like the chemical industry may have asthma often labelled as 'occupational'. Asthma remains a major cause of school and work absence and the health care expenditure on asthma is very high. The Global Initiative for Asthma (GINA) estimates that developed economies might expect to spend 1-2 percent of total health care expenditures on asthma. Approximately 5 per cent of people with asthma have severe asthma. Tragically, 3 people die every day because of asthma attacks and research shows that two thirds of asthma deaths are preventable.
Can asthma be cured?
Although we can control asthma, currently there is no cure for asthma. However, with scientific advancements and the widespread availability of safe and effective treatments, asthma symptoms can be managed well and asthmatic children and adults can lead an otherwise normal life with almost no restrictions.
Why do people get asthma?
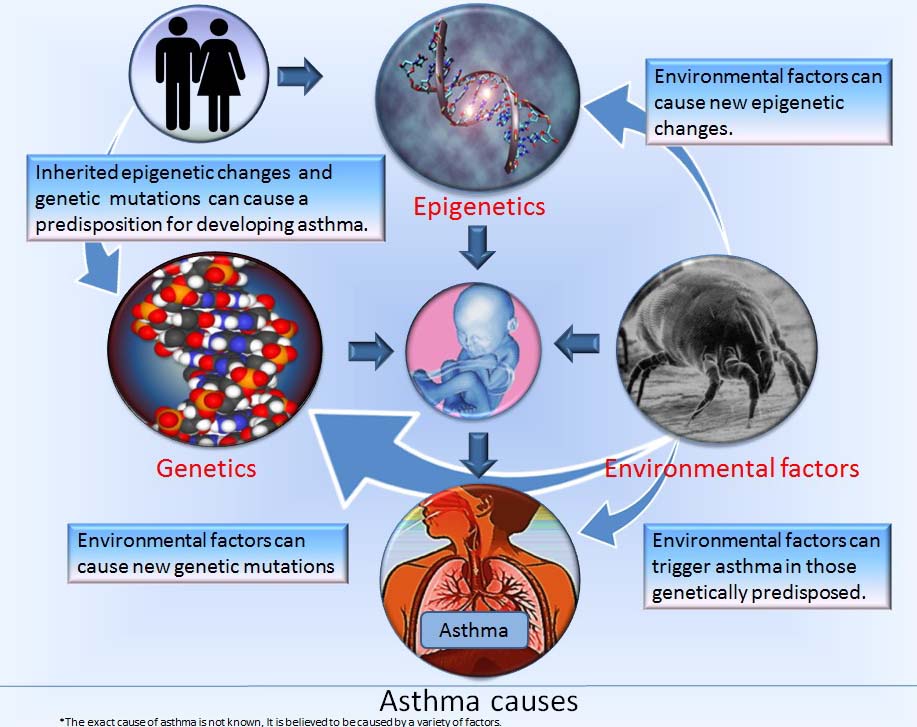
Although we have understood what might trigger asthma, the exact reasons why one gets asthma is not fully understood. Extensive research indicates that a number of factors either alone or in association with other factors can play a role in initiating asthma.
As asthma (and allergies) runs in families, a genetic basis is possible and having parents with asthma increases the risk of asthma in their children. Babies born premature and who weigh less have a tendency to develop asthma. Those with allergies (food, eczema or hay fever), also known as ‘atopic’, have an increased risk of developing asthma. ‘Atopic march’ is a term often used to describe a small child with early onset eczema developing food allergy, and subsequently at a later age, hay fever, and then asthma. Smoking during pregnancy and around the baby or the child increases the risk of asthma.
Others factors include a respiratory illness (Bronchiolitis) caused by a virus called Respiratory Syncitial Virus (or RSV) in early childhood especially if it recurs frequently. Occupational exposure ( to chemicals or dust) and environmental pollution (traffic and industry) may also play a part in this asthma epidemic. There is some evidence that children living near very busy roads are more likely to develop asthma. Female hormones like oestrogen may also play a role in the development of asthma.
Nevertheless, despite extensive evaluations, the cause for asthma in a given child is often unknown.
The ‘Hygiene Hypothesis’
There has been a substantial research evidence that babies are not being exposed to friendly bacteria as we live in cleaner and more urban environments. Proponents of this hypothesis have suggested that such lack of exposure results in altered and lowered immunity and hence might lead to asthma. However, more recent research has been somewhat sceptical of this concept. Nonetheless, it is good to remember that good hygiene practice is helpful in avoidance of asthma triggers and also helps in prevetating the vulnerable child from other diseases.
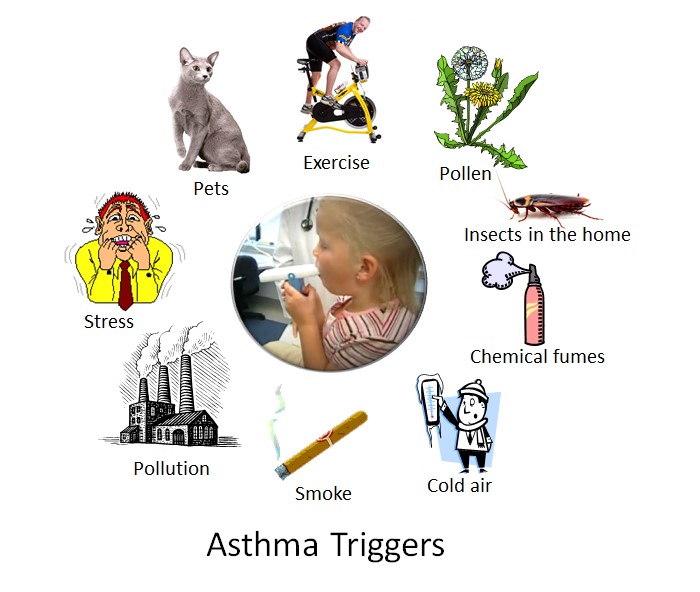
Asthma triggers
We breathe what is around us. Apart from the skin, he nose and the lungs are the only part of the body that comes in close contact with these external agents. Most common asthma triggers include exposure to an agent to which the child is sensitised to. This may be animals and pets, house dust mite, mould and fungi, grass, weeds and trees. Fortunately much of this may be diagnosed by using specialist tests and the allergens may be avoided to a great extent. On the other hand, triggers such as viral infections (colds and flu), exercise and emotional states (depression and laughter). Cold weather, pollution and exposure to smoke may also trigger asthma symptoms.
Diagnosing asthma in a child
Often it is difficult to diagnose asthma as unlike many other conditions there is no single test but it is a process of pattern recognition that only comes by experience. However, you should be alerted if you spot these signs (courtesy Asthma UK).
Cough
A cough that won’t go away or keeps coming back. A night time/early morning cough – this is common in children with asthma. A cough after doing exercise or being active.
Wheeze
A whistling sound when they breathe.
Tight chest
A ‘tummy ache’ is how children might describe it. They might rub their tummy or chest.
Breathlessness
Listen for fast breathing. Watch to see if they’re using lots of their body when they breathe – for example shrugging their shoulders up and down.
Asthma diagnosis
Whilst useful in older children and in adults, in the young child, asthma is diagnosed primarily clinically i.e. by taking a careful and focussed history, thorough examination and assessing response to treatment. Some tests may be undertaken but it is intended in ruling out other conditions that may mimic asthma. These specialist investigations may include a Chest X Ray, allergy tests and lung function assessments (Spirometry)
Asthma treatment
Fortunately, a lot of advancement in the field of medicine has made it possible to control asthma so that a normal life can be expected. This may include asthma education, avoidance (if possible) of potential triggers, inhalation therapy and the use of systemic anti-inflammatory agents (also known as steroids). It is needless to say here that asthma medications are extremely useful and they save lives. However, they have to be taken correctly and consistently (Asthma education).